|
|
Winter 1995 (3.4)
Pages 54-58The Crisis of Beta Thalassemia
in Azerbaijanby Dr. Azer Karimov and Dr. Chingiz Asadov
Institute of Hematology and Blood TransfusionSome people complain that health conditions have deteriorated drastically since independence. But the truth is that we've always had problems. Our equipment is so old-most of it 20 to 30 years old. It's been neglected for a long time not just these last few years. Besides, it's often of very poor quality. We always preferred Czech or East German equipment over the Soviet when we had the choice.
When I used to visit hospitals in Moscow, I saw only American and Western European equipment. With oil money that should have been channeled into Azerbaijan, they bought themselves good equipment and handed off the poor leftovers to our Republic. Occasionally, an Azerbaijani had enough clout with the Central authorities to help us get some decent equipment.
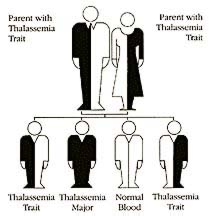
Heredity patterns for Thalassemia. "Trait" means person is carrier and can give disease to offspring even though he or she may not have any symptoms of disease. If both parents are carriers, there is a 25% chance that a child will have the disease. Courtesy: Thalassemia International Federation.
No Blood Bags
Admittedly, we have never faced the kind of crisis we're experiencing with thalassemia today. There are 2,000 children in Azerbaijan who have inherited this blood disorder which causes severe anemia. That's a relatively small number when compared to our population of 7.5 million, but it's a high incidence for thalassemia and the problems it brings to its victims and their families are huge.
Left: Children born with thalassemia, a type of blood disorder, must receive blood transfusions about once or twice a month. This child is receiving a Desferal treatment for the removal of excess iron from her blood. Desferal pumps usually are worn 8-10 hours each day, 4 to 7 days a week for life. Too much iron in the blood can lead to severe complications and death. Research is underway to find a way to administer iron chelation orally instead of by needle. Courtesy: Cooley's Anemia Foundation.
To survive, thalassemic children need transfusions of two to four liters of blood about twice a month. It's a lifelong process that usually begins sometime in the first year of life. And it's a staggering amount of blood for Azerbaijan. It means we need 12 to 13 tons of blood each year just to treat thalassemia-not to mention leukemia, hemophilia, anemia or complications that arise during childbirth, nor the traumatic accidents that we must always be prepared for. Fortunately, there is a cease-fire agreement now so we aren't having to cope with additional war-inflicted injuries and casualties.
Trying to orchestrate this desperate need for blood creates immense logistic problems. Take the first step-collecting blood. These days we don't have blood bags. Since we don't manufacture them, we have to import them. But they're too expensive. For thalassemic patients alone, we need about 26,000 bags with double chambers which cost about $5 a piece. Five dollars might seem like an insignificant sum to a Westerner, but for us, it makes the cost of a single plastic bag equivalent to about half of a doctor's monthly government salary. Without blood bags, we can't transfuse and if the children don't get red blood cells with hemoglobin, they die because their cells don't get the necessary oxygen. It's as simple and as cruel as that.
On average, these children live to be 10-12 years of age in Azerbaijan. In the past, when they received blood transfusions regularly, they reached 15 or 16. The picture is less grim in other parts of the world. In the U.S., for example, the four oldest thalassemic patients - two men and two women - have just celebrated their 43rd birthday this year. But in Azerbaijan, our oldest thalassemic patient is 24.
It's only natural that families can't comprehend that we don't have blood. Only two or three years ago, they could receive transfusions rather easily for their children. Families think we're hiding blood from them. But to be honest, we are collecting only a few liters of blood each day for the entire capital. With no blood bags, we have to collect blood in glass jars. Of course, there are always people who capitalize on others' misfortunes and offer blood at exorbitant sums.
Blood Donors
During the Soviet period, we used to have Blood Donor Groups. The Director of every major organization and institute had the responsibility for collecting a specific amount. You might call it an "obligatory volunteer" system, but it generally worked.
We know that in Western countries people are proud to donate blood. But here they try to conceal it, somehow feeling that it isn't very prestigious. There was one extraordinary exception-Black January 1990, when the Russians attacked Baku. People stood in line demanding to give their blood-even old pensioners. Some even collapsed only to turn around and offer again. If our nation proved itself back then in a difficult situation, we can do it again. Our task at the Institute must be to convince people that blood is needed, not only in extreme situations, but on a daily basis.
But even among our regular donors, we're having difficulties these days. Because of widespread poverty, people aren't getting enough nourishing food. Sometimes they come in to offer blood and we discover their own hemoglobin counts are too low.
Protecting the Blood Supply
But collecting blood is only the beginning of the story. Transfusions require clean blood, free from infectious diseases. Fortunately, we have access to disposable syringes. But we have to test each sample for hepatitis B, AIDS, and syphilis. "Doctors Without Borders" a humanitarian relief agency from Belgium, is currently providing these tests. Fortunately, AIDS is almost non-existent in our country although we have identified a few carriers among our donors. Homosexuality and prostitution are not very widespread and illicit drugs are more likely to be smoked (opium) than injected. All these behaviors help to minimize the risks of AIDS.
Some German companies, namely Diamed, Biotest and Biofac have assisted us in a project initiated by Rafiga Sadigova, the wife of our Ambassador in Bonn.
We used to receive considerable assistance from Relief International (based in Santa Monica, California) for syringes, medication and supplies, but now since they receive a portion of their funding from the U.S. government, they've cut us off. Items like plastic gloves are now going to medical personnel who are not nearly at risk as much as we are. (See discussion this issue about "Freedom Support Act", Section 907 which denies humanitarian aid to the Azerbaijan government in the "Diplomatic Interview" with U.S. Ambassador, Richard Kauzlarich).
Solutions for Thalassemia
For Azerbaijan, the solution to the thalassemia crisis must be organized in stages. We have to find a balance between trying to solve day to day problems while making long range plans.
First of all, we have to renew our list of patients. When people don't find blood, they stop coming, especially from the regions. We need up-to-date equipment such as centrifuges as well as large volume freezer refrigerators. We only have three or four in the entire city but they're 20 years old and often break down and require repair.
Thalassemic patients don't need plasma, only red blood cells so filters are essential to separate the red blood cells from whole blood. As well, we desperately need the iron-chelating agent, desferrioxamine, usually called by its brand name, "Desferal". When a person has many transfusions, too much iron accumulates in his blood causing complications that can damage the heart, liver, pancreas, endocrine systems and ultimately lead to death. Desferal reduces this risk but the drug has to be introduced via a needle inserted under the skin in the abdomen and worn 8-10 hours a day, five to seven days a week. We need about 200-300 of these pumps which cost about $1,000 each.
Another major problem has arisen now that international humanitarian aid is being given in Azerbaijan. There is no designated Center that coordinates these donated medical supplies to really identify needs.
Sometimes items get delivered to private agencies which don't have much experience or which lack medical training. In relation to thalassemia, there have been cases when these rare blood bags, for example, have ended up being sold at drug stores simply because thalassemic recipients didn't know how to find blood donors. In desperation, they gave up treatment and sold the bags. Aid needs to be channeled into facilities which have the capability of overseeing and monitoring treatment from beginning to end so that patients have access to everything in one place and won't have to run frantically all over town when an emergency arises.
Ultimate Solution-No Babies
Ultimately, the solution for thalassemia is for these children not to be born. Theoretically, there are several ways to do this. Couples could be tested prior to marriage. If that were not possible, screening should be offered to examine the pregnant woman to determine if she is a carrier. If so, the father could be tested, too. If they both carry the gene, there is a 25% chance that the child will be thalassemic; 50% chance that it will be a carrier and 25% chance that it will be normal.
Technology does exist for prenatal diagnosis during pregnancy. Unfortunately, we don't yet have this capability at our Center. But even prenatal diagnostics would be very difficult to carry out in Azerbaijan. In Italy, 95% of all thalassemic cases fall into two categories. In Azerbaijan, 20 different forms of thalassemia have been identified. Different forms mean there may be different variations of the DNA which means different reactives would be needed to detect it. In Azerbaijan, approximately 67% of cases are genetically identical to the Mediterranean thalassemia, but we also have cases that are indigenous to types in Iran, Turkey, Africa and India. There even seems to be one genetic combination specific only to Azerbaijan, crossroads between many countries in the region for many centuries, even millennia.
The Future
The only known treatment for thalassemia is bone marrow transplantation. Guido Lucarelli of Pesaro, Italy, is considered the most experienced bone marrow operation specialist related to thalassemia. But finding a perfect bone marrow match is extremely difficult. Occasionally, you'll find a brother, sister or even a parent. But that's about all. It's an expensive operation and still quite risky. A person has a 5-20 percent chance of dying from complications of the transplant and a 5-15 percent chance that the transplant will not work.
We, too, were planning to set up a bone marrow transplant center and the government had already allocated funds. In 1992 we had even signed a contract with a German company to purchase equipment. But then, the war became so intense and the refugee problem crowded out our plans. Now we wait.
Survival is not the solution for the victims of thalassemia. We have to find ways to provide quality life for these children and to support the families, who easily become devastated morally and financially. An Association of Parents with Thalassemic Children has now been formed to develop a transfusion list so that each patient can be pre-scheduled for a specific day each transfusion cycle. Then there wouldn't be a panic for blood. Such a program would alleviate immense complications for families who travel hundreds of kilometers only to be turned away empty-handed.
We'd also like to set up a program to match donors with specific thalassemic children. If a donor felt personally responsible for a specific child, treatment would be more consistent and the donor would also gain more satisfaction.
Scientists expect a cure for thalassemia within eight to ten years, possibly earlier. They're trying to develop a pill that would safely and conveniently remove excess iron from the blood and replace the Desferal pump. Ultimately, they expect the cure to come via gene therapy so patients could be able to produce hemoglobin for themselves. Our task is to provide hope and support to these young people and their parents until that day arrives.
Dr. Azer Karimov is Director of the Institute of Hematology and Blood Transfusion at M. Gashgai Street 87, Baku 37000. Tel: 99412-96-53-18; Fax: 96-63-34. Dr. Chingiz Asadov is former Director and one of the leading physicians at the Center. Mr. Geno Bianco, of Los Angeles, Former President of the California Chapter of Cooley's Anemia (Thalassemia) Foundation, also contributed to this article.
From Azerbaijan International (3.4) Winter 1995.
© Azerbaijan International 1995. All rights reserved.Back to Index AI 3.4 (Winter 1995)
AI Home | Magazine Choice | Topics | Store | Contact us